The Department of Education (DepEd) issues DepEd Memorandum with Limited Application No. 1, s. 2021 dated September 15, 2021, on the Conduct of School Safety Assessment in Preparation for the Conduct of Pilot Implementation on Face-to-Face Learning Modality for the 638 Pre-Identified Schools.
Table of Contents
Conduct of School Safety Assessment in Preparation for the Conduct of Pilot Implementation on Face-to-Face Learning Modality for the 638 Pre-Identified Schools
The Department of Education (DepEd), in its commitment to ensure learning continuity amid the challenges and ambiguities brought about by the COVID-19 pandemic, issues the School Safety Assessment Tool (SSAT) to assess the readiness of schools to participate in the conduct of the pilot implementation of face-to-face learning modality. In preparation for the reopening of the schools, the SSAT, which was initially issued as School Readiness Checklist last December 2020 through an Office Memorandum, aims to reassess the readiness of the 638 pre-identified schools.
In view of the current context of the schools, the SSAT shall be redeployed to gather data and information on the schools’ present situation and conditions relevant to safe reopening of schools. The data gathered shall be used as baseline information in preparation for the implementation of the face-to-face learning modality. This is in line with the Department’s effort to reopen the schools while ensuring that the health, safety, and well-being of learners, teachers, and personnel remain as its utmost priority.
The SSAT focuses on four main areas, namely: (1) Managing School Operations, (2) Focusing on Teaching and Learning, (3) Well-being and Protection, and (4) Home-School Coordination. It contains indicators and standards that would show readiness of the schools to participate in the pilot study of the face-to-face learning modality if met.
The School Heads shall accomplish the SSAT on or before September 20, 2021, and ensure that transparency and honesty are observed by conducting consultation with the key stakeholders. The Schools Division Office (SDO) shall facilitate the administration of the tool to the nominated schools and must validate the submitted results. The Regional Office (RO) shall facilitate the approval and transmittal of the list of the qualified schools in their respective regions to the Office of the Director – Planning Service, through the Education Management and Information System Division (EMISD).
In view of the foregoing, the following enclosed documents are issued for guidance and reference:
a. Enclosure No. 1 – Process Flow of the Data Collection and Report Generation for SSAT
b. Enclosure No. 2 – Details on the Orientation for the SDO and RO Personnel on the Administration of SSAT
c. Enclosure No. 3 – School Safety Assessment Tool (2021) for the Pilot Study on Face-to-Face Learning Modality
All concerned ROs and SDOs are urgently enjoined to ensure immediate and widest dissemination of the SSAT in schools.
For queries or concerns, please contact the Bureau of Human Resource and Organizational Development – School Effectiveness Division (BHROD-SED) through email at bhrod.sed@deped.gov.ph.
Immediate dissemination of this Memorandum is desired.
Process Flow of the Data Collection and Report Generation of the School Safety Assessment Tool
To ensure smooth implementation of the tool, procedures on the Data Collection and Report Generation are stated below.
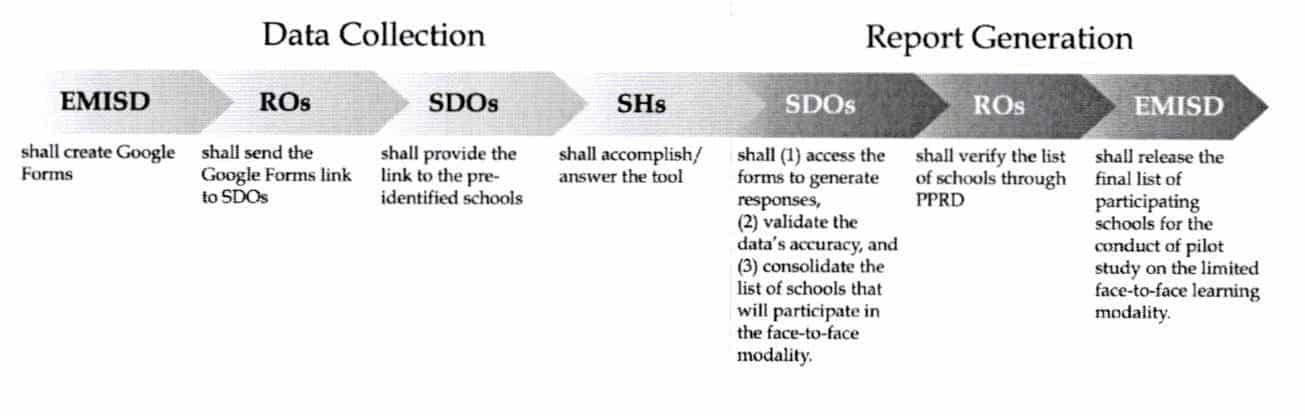
On Data Collection
The Regional Offices (ROs) shall disseminate the information on the accomplishment of SSAT to the Schools Division Offices (SDOs). The SDOs shall inform the schools in their divisions that are included in the list of 638 pre-identified schools which passed the initial assessment conducted last December 2020 to accomplish the SSAT using the link assigned to their regions.
In accomplishing the tool, the School Heads (SH) shall ensure that honesty and transparency are observed and key school stakeholders are consulted. The SSAT shall only be accomplished through the Google Forms link provided to them by their SDOs.
On Report Generation
The SDOs shall be given access to the back-end data of the schools that accomplished the SSAT to generate school-level responses and validate its accuracy.
In case the schools submit multiple responses, the SDOs shall consider the latest responses as final.
The concerned SDOs shall create a composite team with the following members: (a) Disaster Risk Reduction and Management (DRRM) Coordinator, (b) SDO Health Personnel, (c) Planning Officer, (d) SDO Engineer, and (e) a representative from the Curriculum Implementation Division (CID), who shall conduct monitoring visit to validate the data and verify the results submitted by the schools.
During the monitoring visit, safety protocols must be observed. The SDO’s composite team and up to five (5) school personnel shall be present in school.
For schools that met all indicators, the SDOs shall validate the veracity of the data submitted. In the event that the SDOs find issues on the validity of data submitted by the schools, i.e., unmet indicators that were identified as met, SDOs shall provide technical assistance to help the school/s meet all indicators to ensure their participation in the pilot implementation of the face-to-face learning modality. In case the schools are not able to meet all indicators prior to the conduct of the pilot implementation of the face-to-face learning modality, the SDOs shall continuously provide technical assistance to help them prepare for the expanded implementation of the face-to-face learning modality.
After the conduct of monitoring visit, the SDOs shall finalize the data submitted by the schools by updating data entries if applicable, i.e., unmet indicators that are identified as met. Upon finalization of the data, the designated focal person of the SDOs shall consolidate the list of schools that meet all indicators and will qualify to participate in the limited face-to-face learning modality. The said list must be forwarded to the PPRD of their respective Regional Offices.
For schools that did not meet all indicators, the SDOs shall inform them of their unmet indicators and shall provide technical assistance to help them prepare for the expanded implementation of the face-to-face learning modality. They shall provide progress update on the accomplishment of SSAT by adding the schools’ latest data in the database every two weeks after the deadline, September 20, 2021. This is to monitor the number of schools prepared to participate in the implementation of the succeeding phases of the face-to-face learning modality.
The PPRD of ROs shall submit in a designated Google Sheet the final responses and list of qualified schools for the limited face-to-face learning modality to the Office of the Director – Planning Service (PS-OD), through the Education Management Information System Division (EMISD).
EMISD shall consolidate the list submitted by the Regional Offices and coordinate with PS-OD to release the final list of schools that will participate for the pilot implementation of the face-to-face learning modality.
For the links of the Google Forms per region, kindly refer to the matrix below:
| Region |
|---|
| I |
| II |
| III |
| IV-A |
| IV-B |
| V |
| VI |
| VII |
| VIII |
| IX |
| X |
| XI |
| XII |
| CARAGA |
| NCR |
| CAR |
The schools shall accomplish the SSAT on or before September 20, 2021. Kindly see Enclosure No. 1 for the Process Flow for Data Collection and Report Generation Process of this memorandum, and Enclosure No. 3 for the School Safety Assessment Tool. Furthermore, the conduct of the monitoring visit by the composite team from the SDOs shall take place on September 22-29, 2021.
Details on the Orientation for the SDO and RO Personnel on the Administration of SSAT
To guide the SDOs and ROs in providing technical assistance to the schools, an orientation shall also be conducted on the following dates with respective MS Teams link:
| BATCH | DATE | REGION | SDOs | TARGET PARTICIPANTS |
|---|---|---|---|---|
| BATCH 1 | September 16, 2021 Time: 1:30 p.m. – 5:00 p.m. | I | SDO Alaminos City SDO Dagupan City SDO Ilocos Norte SDO Ilocos Sur SDO Pangasman II SDO Vigan City | Planning Officer from Regions I, II, III, IV-A, IV-B, V, VI, NCR, and CAR (1) SDO Health Personnel and (1) DRRM Coordinator |
| II | SDO Batanes SDO Cagayan SDO Cauayan City SDO Hagan City SDO Isabela SDO Nueva Vizcaya | |||
| III | SDO Aurora SDO Gapan City SDO Nueva Ecija SDO Zambales | |||
| IV-A | SDO Quezon | |||
| IV-B | SDO Calapan City SDO Marinduque SDO Occidental Mindoro | |||
| V | SDO Albay SDO Camarines Norte SDO Camarines Sur SDO Catanduanes SDO Iriga City SDO Ligao City SDO Masbate SDO Masbate City SDO Naga City SDO Sorsogon City SDO Tabaco City | |||
| CAR | SDO Abra SDO Benguet SDO Ifugao SDO Kalinga SDO Mountain Province SDO Tabuk City | |||
| NCR | SDO Caloocan City SDO Las Pinas City SDO Makati City SDO Muntinlupa City SDO Parahaque City | |||
| VI | SDO Iloilo SDO Aklan SDO Antique SDO Bacolod City SDO Bago City SDO Cadiz City SDO Escalante City SDO Guimaras SDO Kabankalan City SDO Negros Occidental SDO Passi City SDO Roxas City SDO Sagay City SDO San Carlos City SDO Sipalay City | |||
| BATCH 2 | September 17, 2021 Time: 1:30 p.m. – 5:00 p.m. | VII | SDO Bais City SDO Bayawan City SDO Bohol SDO Cebu Province SDO City of Bogo SDO Guihulngan City SDO Negros Oriental SDO Siquijor SDO Tagbilaran City | |
| VIII | SDO Calbayog City SDO Leyte SDO Samar SDO Southern Leyte | |||
| IX | SDO Dapitan City SDO Dipolog City SDO Isabela City SDO Pagadian City SDO Zamboanga City SDO Zamboanga del Norte SDO Zamboanga del Sur SDO Zamboanga Sibugay | |||
| X | SDO Bukidnon SDO Cagayan de Oro SDO Camiguin SDO El Salvador City SDO Gingoog City SDO Lanao del Norte SDO Malaybalay City SDO Misamis Occidental SDO Misamis Oriental SDO Oroquieta City SDO Ozamiz City SDO Valencia City | |||
| XI | SDO Davao de Oro SDO Davao del Sur SDO Tagum City | |||
| XII | SDO General Santos City SDO Kidapawan City SDO Koronadal City SDO North Cotabato SDO Sarangani SDO South Cotabato | |||
| CARAGA | SDO Agusan del Sur SDO Agusan del Norte SDO Bayugan City SDO Bislig City SDO Butuan City SDO Cabadbaran City SDO Dinagat Islands SDO Surigao City SDO Tandag City SDO Siargao SDO Surigao del Norte SDO Surigao del Sur |
For confirmation of attendance to the online orientation, please accomplish the online confirmation form through the link.
For queries or concerns, you may contact the Bureau of Human Resource and Organizational Development – School Effectiveness Division (BHROD-SED) through email at bhrod.sed@deped.gov.ph.
DepEd School Safety Assessment Tool (2021) for the Pilot Study on the Face-to-Face Learning Modality
The School Safety Assessment Tool (SSAT) shall be used to assess the readiness of the schools to participate in the conduct of the pilot implementation of face-to-face learning modality in the time of the COVID-19 pandemic. The data gathered shall be used as baseline information in preparation for the safe reopening of classes.
School Name:
School ID:
Division:
Contact Number:
For the past twenty-eight (28) days, has the barangay where your school is located recorded any confirmed COVID-19 case/s? Kindly refer to your respective barangay for the data.
Is the school accessible through public transportation? Specify mode of transportation.
Is the school accessible through walking?
If the barangay where the school is located has not recorded any confirmed COVID-19 case/s in the past 28 days, and the school is accessible by public transportation or walkable, proceed in answering this safety assessment tool, otherwise, your school cannot be nominated as a participating school for the implementation of limited face-to-face learning modality.
For a school to be eligible for the implementation of the face-to-face learning delivery modality, they need to meet all the indicators (YES to all indicators). In answering the SSAT, School Heads shall ensure that key stakeholders are consulted. The Schools Division Office (SDO) shall facilitate the administration of the tool to the nominated schools and shall create a composite team who will conduct monitoring visits to validate the data and verify the results submitted by the schools.
Managing School Operations
I. Shared Responsibility
- The school has secured support of LGUs (Barangay, Municipality, City, Province) through a resolution or a letter of support.
- The school has secured written consent from parents/guardians who will participate in the limited face to face classes.
- The school has mobilized resources and support from community stakeholders to meet the standards of the health and safety protocols.
- The school has conducted simulation activities among school personnel regarding protocols and routines to replicate and discuss possible scenarios during the actual conduct of face-to-face classes.
II. Alternative Work Arrangement
- The school has implemented an Alternative Work Arrangement necessary to deliver quality basic education in a safe learning environment to learners.
a. Number of teachers who physically report meets the required teacher: learner ratio
b. Teachers who physically report are 65 years old and below
c. Teachers who physically report to not have comorbidities, immunodeficiency, or any health risk/conditions
d. Teachers who have service vehicles from and to area of residence and school e. Teachers who physically report are from within the city/municipality where school/learning center is located.
- The school has oriented teaching personnel and nonteaching personnel on the Alternative Work Arrangement that will be implemented during the limited face-to-face classes.
III. Classroom Layout and Structure
- The school has established mechanisms inside the classroom to ensure zero to minimal risk of COVID-19 transmission of the learners.
a. Number of seats to be occupied must not exceed from the required number of maximum learners in the classroom
b. Seats to be occupied must be at least 1-2 meters apart
c. Numbers of seats shall be equivalent to the number of learners present
d. Presence of markers and stickers on the floor to manage traffic system and physical distancing inside the classroom
e. Availability of working electric fans
f. Open windows and doors at all times
g. Installation of appropriate ventilation equipment such as general and exhaust ventilation and CO2 monitoring devices
h. Availability of a sterilization box where outputs (e.g., quiz papers) submitted by the learners will be placed for disinfection
i. Usage of high-efficiency particulate air (HEPA) filtration air purifiers to clean recirculated air for air-conditioned spaces, provided that the unit is adequate for the size of the room in which it is installed.
IV. School Traffic Management
- The school has set-up clear and easy-to-understand signages, preferably in local languages and Braille, and mechanisms to strengthen observance of health protocols and protective measures.
a. Display of school map at the entrance point indicating the location of the classrooms
b. Designation of separate entrance and exit points in the school
c. Designation of separate entrance and exit points in high traffic areas (unidirectional markers, installation of signages for cueing and unidirectional movement, sectioning, and queueing)
d. Designated entrance and exit points in the classrooms
e. Hallway ground markings for walking direction guide
f. Designation of areas for queue (e.g., restroom, library, principal’s office, etc.)
V. Protective Measures, Hygiene Practices, and Safety Procedures
- The school has established safe entrance and exit procedures for teachers, students, non-teaching personnel, and school visitors.
a. Availability of temperature thermal scanner or thermal gun in entrance and/or exit gates
b. Availability of hand sanitizer or alcohol dispenser in school gates
c. Availability of surgical masks at school entrance reserved for symptomatic individuals
- The school has established a contact tracing procedures/tools for school-goers.
a. Health declaration sheet for school personnel
b. Health declaration sheet for students
c. Contact tracing tool for school-goers
- The school has mobilized the School COVID-19 DRRM team that will take charge in ensuring effective implementation of the school’s health and safety protocols that are in place and are observed during the preparation and implementation of limited face-to-face classes.
a. Designation of a Safety Officer who shall serve as the focal person for the health and safety protocols of the school
- The school has set up a proper sanitation and hygiene facility for school-goers.
a. Availability of handwashing station with clean and safe water supply
b. Availability of clean and safe toilet facilities
c. Schedule of supervised handwashing and toothbrushing activities
d. Placement of handwashing facilities in a strategic location (e.g., school entrance)
e. Placement of trash bins in strategic locations
f. Visuals signages on proper waste management practices near trash bins
- The school has ensured regular sanitation and disinfection of school facilities, furniture, and equipment.
a. Schedule of sanitation of frequently touched surfaces (e.g., table, doorknobs, light switches, etc.) every after end of a school shift
b. Schedule of disinfection of school facilities (e.g., chairs, desk, blackboard, toilet facilities)
c. Availability of sanitation and disinfecting materials
- The school has ensured a proper disposal system of infectious wastes, such as used tissues and masks, in noncontact receptacles.
a. Disposal of all used PPEs in a separate leak-proof yellow trash bag/container with a cover properly labelled as “USED PPE”
b. Collection of the leak-proof yellow trash bag/container regularly or twice a day (after end of class and after working day) from designated/specific area to the general collection area for treatment and disposal
c. Availability of medical-grade face mask required for school personnel when collecting/handling the leak-proof yellow trash bag/container
d. Treatment through disinfection or spraying of the collected wastes with a chlorine solution (1:10) in accordance with DOH Department Memorandum No. 2020-0157 “Guidelines on Cleaning and Disinfection in Various Settings as an Infection Prevention and Control Measure Against COVID-19”
e. Disposal of the disinfected PPE with general waste to the final disposal facility
VI. Communication Strategy
- The school has developed a communication plan.
a. Identification of platform of communication for coordination purposes among the learners, parents/guardians, and teachers
b. Database of contact details including contact number and address of parents/guardians of the learners are kept to inform them in case their child shows flu-like symptoms while in school premises
c. Development of child-friendly Information, Education and Communication (IEC) materials on hygiene practices and respiratory etiquette including hand hygiene (hand disinfection thru handwashing and/or use of 70% isopropyl alcohol), respiratory hygiene and cough etiquette (coughing or sneezing into tissues or one’s elbow), protective measures (proper use of face shield and face mask, physical distancing), among others, that are posted in common areas and are available in local languages and braille
- The school has prepared an orientation session for learners, parents, guardians, teaching and non-teaching personnel, external stakeholders, and LGU of the eligibility criteria for participation, existing protocols, mechanisms, and procedures needed in the conduct of the limited face-to-face classes.
a. Schedule of the orientation (at least one week prior to the conduct of the face-to-face classes)
b. Orientation materials are made available for distribution to teachers, learners, parents, BLGU, DRRM team members, and persons-in-charge in ensuring observance of protocols, mechanisms, and procedures
- The school has a proactive COVID-19 local hotline/help desk or any similar local mechanism that connects and coordinates to the hospitals, testing facilities, and LGUs.
- The school has prepared a re-orientation session for school stakeholders on measures needed for the reopening of the school in the event of resurgences and school lockdown.
VII. Contingency Plan
- The school has followed a decision model and contingency plan for reclosing and reopening the school in case of COVID-19 resurgence in the community.
a. Inclusion of decision points for school lockdown dependent on the assessment and decision of the Local Task Force against COVID-19 (LTF) with the following considerations:
When there is suspected, probable, or confirmed COVID-19 case to facilitate disinfection and contact tracing;
Change in number of community transmission and quarantine risk classification identified by IATF;
Violations/instances of non-compliance of learners or personnel with the minimum public health standards or PDITR for review of protocols
b. In the event of school lockdown, all learners shall revert to distance learning.
c. Implementation of a 24-hour granular lockdown period for disinfection following identification/detection of suspect, probable, or confirmed COVID-19 confirmed case/s, only after which can it be opened for use to occupants.
d. Consideration of the following for the reopening of classes after a school lockdown:
Completed contact tracing
Completed disinfection activities
14 days without confirmed cases in the school
School is in a barangay with low to no community transmission
Area where the school is located is classified as minimal-risk
e. Implementation of return to school/work policies consistent with latest national guidelines
For close contacts:
i. For fully vaccinated individuals: Seven (7)-day quarantine has been completed regardless of negative test result
ii. For unvaccinated or with incomplete vaccination: Fourteen (14)-day quarantine has been completed regardless of negative test result
For suspect, probable or confirmed cases, whether fully vaccinated, unvaccinated, or with incomplete vaccination:
i. For asymptomatic: Ten (10)-day isolation have passed from the first viral diagnostic test and remained asymptomatic throughout their infection.
ii. For mild to moderate COVID-19 confirmed cases: Ten (10)-day isolation have passed from onset of the first symptom, respiratory symptoms have improved (cough, shortness of breath), AND have been afebrile for at least 24 hours without use of antipyretic medications.
iii. For severe and critical COVID-19 confirmed cases: Twenty-one (21)-day isolation has passed from onset of the first symptom, respiratory symptoms have improved (cough, shortness of breath) AND have been afebrile for at least 24 hours without the use of antipyretic medications.
iv. For immunocompromised, do RT-PCR testing on the 10th day. If RT-PCR test results turn out positive, refer to Infectious Disease Specialist. If RT-PCR test results turn out negative, discharge from isolation.
Medical certification or repeat testing is not necessary for the safe return to work of immunocompetent individuals, provided that a licensed medical doctor certifies or clears the patient.
- The school has developed strategies for the continuity of learning while the school is closed until the local authorities have determined the safe resumption of face-to-face classes.
a. Distance learning modalities during lockdown in the decision model and contingency plan
b. Strategies for the reopening of schools after the lockdown in the decision model and contingency plan
Focusing on Teaching and Learning
I. Learning Resources
- The school has secured sufficient supply of learning resources needed for the face-to-face classes.
a. Implementation of 1:1 Student to Self-Learning Module (SLM) to lessen student interaction during class hours
b. Implementation of 1:1 Student to Textbook ratio to lessen student interaction during class hours
II. Limited Face to Face Classes
- The school has designed class program/s that cater both learners of the limited face-to-face classes arrangement and distance education while observing the maximum 6-hour classroom teaching hours of teachers.
a. Arrangement of the number of class sections in a way that each class section will be able to attend face-to-face classes: o Class A: Half-day face-to-face classes in one straight week and other half-day for distance learning o Class B: One straight week of pure distance learning o Classes shall alternately attend face-to-face classes every week for the whole duration of the pilot implementation
b. Class program indicating specific schedule/breakdown of hours for the face to face classes including staggered start and close of the school day per grade level
c. Class program indicating specific schedule/breakdown of hours for distance learners including staggered start and close of the school day per grade level
d. Class program indicating schedule of staggered break time hours
e. Signages on protocols prohibiting activities that require large gatherings
f. Implementation of the maximum hours of stay of the learners in schools (4.5 hours for Gl-6 learners and 3 hours for kindergarten learners)
- The school has comprehensively profiled learners who will participate in the implementation of the face to face classes.
a. Learners who reside within the city/municipality where the school/learning center is located
b. Learners who can walk their way to school, or ride with available private transport, or with regulated public transportation
c. Learners without existing comorbidities
d. Prioritization of learners who require childcare, such as those whose parents must work outside the home, or who have no directly available and immediately responsible adults/guardians at home
e. Prioritization of learners who are heavily dependent on face-to-face learning interventions, such as Key Stage 1 learners (Kindergarten to Grade 3)
f. Prioritization of learners who struggle to meet required learning competencies
g. Prioritization of Senior High School (SHS) learners enrolled in Technical-Vocational-Livelihood (TVL) track requiring workshop equipment in school
h. Prioritization of learners that are documented to be affected by mental health concerns that may be eased by face-to-face interactions
- The school has ensured an attendance monitoring of learners to determine which participating learners are exhibiting difficulties in coming to school and which learners who cannot participate in face-to-face classes will revert to full distance learning.
- The school has informed teachers to conduct consultations with parents, provision of feedback and instructional support for learners, facilitation of assessment, preparation of Weekly Home Learning Plan (WHLP), and other related tasks after face to face classes.
- The school has ensured prohibition of conduct of physical or face-to-face large gatherings, group work, or activities that will require close contact or where physical distancing may not be possible (e.g., school activities, field trips, sports festivals, flag ceremonies).
III. Teacher Support
- The school has provided an appropriate learning and development support plan in providing better quality basic education services.
a. Learning and Action Cells (LAC) sessions highlighting provision of remediation/intervention for learners during the face-to-face classes
b. Coaching, mentoring, and training relevant in facilitating blended learning approach
- The school has oriented teachers on their budget of work and ensured that the school requirement for the learners is in observance of academic ease.
a. Orientation on the implementation of the Most Essential Learning Competencies (MELCs) included in their budget of work during the limited face-to-face classes
b. Orientation on the observance of academic ease and provision of flexibility to learners in managing limited face-to-face classes
Well-Being and Protection
I. Personal Protective Equipment
- The school has secured sufficient supply of personal protective equipment (PPEs) for learners and school personnel.
a. 1:1 Face mask to Person (daily) ratio
b. 1:1 Face shield to Person ratio
c. 1:1 Toothbrush and Toothpaste to Learner ratio (K-6 learners)
d. 1:1 Bar of soap to Learner ratio enough for 5x of handwashing per day (K-6 learners)
e. Availability of emergency health kits that include PPEs and other needed supplies and materials in the school clinic
f. Availability of PPEs for COVID-19 team members, health personnel, and maintenance, and security guards
- The school has secured adequate supply of face masks, face shields, and/or other COVID-19 protective gears for learners.
a. 1:1 Replacement of lost and damaged PPE to Person ratio
- The school has ensured that the available sanitation and disinfection materials are approved by the Philippine Food and Drug Administration (FDA) such as:
a. Sodium hypochlorite recommended ratio of 0.1% (1000 ppm) by dissolving % tsp of chlorine or 2 g to 2L of clean water for regular disinfection, and recommended ratio of 0.5% (5000 ppm) for body fluids by dissolving 1 tbsp of chlorine or 10 g to 2L of clean water
b. Ethanol in all surfaces at a recommended ratio of 70-90%, or
c. Hydrogen peroxide in all surfaces at a recommended ratio of >0.5%
- The school has secured sufficient supply of sanitation and disinfection materials for strategic school locations.
a. 1:1 bottle of hand-sanitizers/alcohol-based solutions/other disinfectants to restroom
b. 1:1 bottle of hand-sanitizers/alcohol-based solutions/other disinfectants to classroom
c. 1:1 bottle of hand-sanitizers/alcohol-based solutions/other disinfectants to entrance/exit point
- The school has ensured PPE requirements, specifications, and standards for different types of COVID-19 management activities in accordance with DOH DM 2020-0176A.
a. Availability of medical mask and face shields for triage and screening of individuals in points of entry (for personnel in school entrances)
b. Availability of medical mask, goggles or face shield, gloves, gown for caring for a suspected case of COVID-19 with no aerosolgenerating procedure (for personnel in school clinics)
c. Availability of respirator (N95 or FFP2), goggles or face shield, gloves, gown for caring for suspected/confirmed cases of COVID-19 with no aerosol-generating procedure for personnel in school clinics)
d. Availability of full PPE for assisting in transporting passengers to a healthcare facility
II. COVID-19 Case Management
- The school has developed strategies to prevent COVID-19.
a. Conduct of hand hygiene and temperature checks using a thermal scanner prior to entering the school
b. Prioritization of non-face-to-face communications and coordination through available platforms and discouragement of entrance of school visitors and other external stakeholders
c. Conduct of daily rapid health checks in the classroom
d. Conduct of necessary disinfection activities especially in the areas of the school frequented by personnel or learners that tested positive
e. Availability of surgical face masks and school clinic for further assessment of anyone who will show symptoms of COVID-19
f. Establishment/setting-up/refurbishment of a school clinic to provide basic health services to all school-goers, such as:
Health assessment and physical examination, as needed
Appropriate intervention, first aid, or treatment
Proper management of symptoms, including rest at home
Referral and follow-up of learners, teachers, and personnel to appropriate facilities
g. Designation of private screening area at the entrance where school-goers who show symptoms upon screening can be further examined, or referred
h. Designation of separate space where sick school-goers who have been managed in the clinic can temporarily stay, awaiting referral to the appropriate health facility, without creating stigma
i. Designation of clinic teachers(s) in absence of school health personnel, who shall provide basic health services and facilitate referral in coordination with the school health personnel at SDO, in absence of school-based health personnel
j. Orientation to the clinic teacher by the school health personnel at the SDO for proper guidance on how to effectively run the school clinic
k. Reiteration of protocols for learners, teachers, and personnel who manifest COVID-19 symptoms to not physically report to school and seek medical advice virtually if possible
l. Record of students’ health status and development, including immunization checks to prevent outbreak-prone vaccine-preventable disease (e.g., measles)
- The school has identified strategies to detect COVID-19.
a. Cooperation with the local health authorities in the tracing and quarantine of close contacts of confirmed cases of COVID-19 consistent with DOH guidelines
b. Presence of the School DRRM Team who shall ensure that contact tracing activities, as required by the local health authorities, are initiated, and completed among the possible close contacts among DepEd personnel and learners
c. Close coordination with Epidemiology Surveillance Unit (ESU) officers per setting
DOH Regional ESU of reporting school
LGU City ESU/Provincial ESU/Municipal ESU of reporting school
DOH Regional ESU of identified case (place of residence) o LGU City ESU/Provincial ESU/Municipal ESU of identified case (place of residence)
d. Development of a reporting system requiring parents to report to the school if their children are experiencing flu-like system, recommendation of testing to be done immediately with support and guidance from the LGUs
e. Provision of health form to parents/guardians at the beginning of each school term confirming their child and/or family members do not have COVID-19 before being permitted to go to school to be submitted 24 to 72 hours prior to the start of school opening
- The school has developed strategies to isolate and treat COVID-19.
a. Designation of rooms for isolation of students and personnel with fever and flu-like symptoms near the entrances
b. Availability of transport vehicles from school to Temporary Treatment and Monitoring Facility (TTMF)
c. Notification of family member/guardians of the learner, or family member of school personnel who show flu-like symptoms
d. Immediate isolation and referral of the personnel/s or learner/s who show COVID-19 symptoms based on the severity for proper management and appropriate testing
e. Provision of necessary emergency care to the personnel or learner following precautionary measures, by the health personnel or designated clinic teacher
f. Referral/full disclosure of the case to the identified health authority (e.g., barangay health station, rural health unit) for further evaluation or referral to a hospital if needed
g. Strict observance of advice from health authorities including possibility of home quarantine or isolation in a quarantine facility or confinement
h. Report of the close follow-up of the attending/assigned school health personnel or designated clinic teacher with the condition of the identified learner/personnel to the SDO School health and Nutrition Unit/Section, as required by existing reporting mechanisms
i. Strict compliance of learners and personnel who have tested positive for COVID-19 to not return to school without clearance from medical authorities
j. Monitoring and provision of necessary support of the School Head (SH) to all cases (close contacts, suspect, probable, confirmed)
k. Coordination of SH to all cases with DepEd school health personnel and local health authorities
l. Coordination of SH with the SDO in ensuring continuity of teaching and learning in line with the school’s contingency plan
m. Strict observance of provision of Section IV.A (Screening of Returning Personnel and Learners and Testing Protocol) of the Specific Measures for COVID-19 Prevention and Mitigation in Schools (Enclosure No. 2 to DepEd Order No. 014, s. 2020) before the participation of COVID-19 infected learners or personnel in the face to face classes
- The school has developed strategies in providing psychosocial support to the learners, teachers, and personnel.
a. Allotment of time and preparation of modules on Mental Health to be facilitated by their respective classroom advisers or designated teachers
b. Designation of trained teachers who will facilitate activities fostering Mental Health such as mental health topics, nature of COVID-19, and preventive measures (WASH, physical distancing, etc.)
c. Setting up of an operational Guidance Office that is staffed by a registered guidance counsellor (RGC) or a designated guidance associate (not an RGC but is trained on MHPSS and is capable of effective referral) every school day, to provide basic mental health services to learners, teachers, and personnel who may need such services
d. Availability of a hotline/online platform in the SDOs to provide counselling services to learners, teachers, and personnel who require counselling services, in absence of an RGC
e. Provision of specialized psychosocial support to learners, teachers and personnel who are confirmed to be positive, under isolation/ quarantine, and categorized as suspect and probable, through the Guidance Office using the DRRMS MHPSS materials as reference
f. Establishment and contextualization of the inter-sectoral referral pathways to ensure that psychosocial needs of both the personnel and the learners are provided
g. Engagement of parents, guardians, or any care providers of learners on taking care of mental health and creating a positive environment
h. Coordination of mechanisms to ensure that the mental health and the basic needs of learners and personnel with pre-existing mental health conditions and special needs including neurologic and substance abuse disorders such as medications and other key services are provided
i. Strict adherence to Republic Act No. 10173 or the Data Privacy Act of 2012 in the provision of mental health services and referral
j. Promotion of “school-life balance” through proper scheduling of schoolwork that will allow learners to enjoy quality time at home
k. Mobilization of trained Psychological First Aid (PFA) providers of the schools to provide necessary mental health and psychosocial support to concerned personnel or learners
- The school has established a clear procedure of referral system for COVID-19 confirmed and suspected personnel and learners.
a. Communication plan which includes coordination system with LGU for school personnel and learners who show flulike symptoms
b. Communication plan which includes a referral system for COVID-19 confirmed and suspected personnel and learners
c. Flow chart of the referral system
- The school has established a clear contact tracing and quarantine system for close contacts of COVID-19 confirmed positive cases.
a. Communication plan which includes coordination system with local health authorities in contact tracing and quarantine of close contacts of confirmed COVID-19 positive cases
b. Communication plan which includes notification of family/parent(s)/guardian(s) of the concerned learner/s
c. Flow chart of the contact tracing and quarantine system
d. Contingency plan for school lockdown
III. Including the Most Marginalized
- The school has identified learners who are most vulnerable and disadvantaged in terms of access to learning as indicated in the eligibility of learners, such as inclusion of:
a. indigent children
b. out-of-school youth
c. physically and mentally handicapped
d. distressed individuals and families, including internally displaced persons (IDPs)
e. low resourced students
f. abandoned and neglected children
g. street children
h. children of former rebels
i. children living in conflict-affected areas and vulnerable communities (CVAS)
j. children with disabilities and SPED students
k. children from Geographically Isolated and Disadvantaged Areas
- The school has identified learners who are most vulnerable and disadvantaged in terms of access to learning as indicated in the eligibility of learners, such as inclusion of:
a. Inclusion of learners who need assistive devices that do not require them to remove their face masks
b. Coordination with partner agencies in the provision of assistive devices such as wheelchairs, cane, walkers, and others
c. Ensured that parent/guardian of learners are informed that his/her child has their own assistive device during face-to-face classes
- The school has developed learning strategies to cater the needs of the marginalized learners such as modules in braille, mother-tongue languages, and usage of Filipino Sign Language.
- The school has ensured participation in school-based services which includes but is not limited to feeding and nutrition programs, immunizations, Mental Health and Psychosocial Support (MHPSS), prevention of Violence against Children (VAC) (i.e., bullying from social stigma) and other health services.
- The school has established close coordination with the Department of Social Welfare and Development (DSWD) Case Managers of those learners who are marginalized; Other partner agencies and organizations such as National Council on Disability Affairs (NCDA).
- The school has coordinated with their respective local government units with the implementation of routine school-based immunization (SBI) and other school health-related services such as but not limited to deworming and weekly iron-folate acid supplementation (WIFA).
a. Routine implementation of SBI together with school health services among target learners
b. Facilitation of the completion of routine immunizations through regular immunization mechanisms available through the National Immunization Program (NIP)
c. Routine immunization card checks through the school nurse or the designated clinic teachers to ensure that children entering schools have completed their routine immunization (i.e., 3 doses of Polio and DPT-HepB-Hib vaccines, and two doses of Measlescontaining vaccines) in the community
d. Referral of learners who have not completed their routine infant vaccines to the nearest LGU/private pediatrician for catch-up vaccination
e. Participation in intensive health promotion campaign activities/supportive-policies that shall be instituted by schools in collaboration with their local health offices to maintain optimal health-seeking behaviors of learners and other community members
Home-School Coordination
- The school has developed a plan in coordinating with the Barangay Local Government Unit (BLGU) or the Barangay Health Emergency Response Team (BHERT) in ensuring that protocols are observed properly.
a. Operationalization of the Preventative Alert System in Schools (PASS) for COVID-19 (per DepEd Memorandum No. 15, s. 2020)
- The school has developed a strategy in orienting parents on health protocols and safety measures.
a. Safe drop-off and pick-up procedures
b. Safety precautions and preventive measures while commuting [e.g., wearing of proper face masks and face shields, refrain from talking and eating while in public transportation, ensure adequate ventilation, frequent and proper disinfection, appropriate physical distancing]
c. Safety precautions and preventive measure upon entering the school premises
- The school has identified a designated waiting area with proper ventilation for parents/guardians.
Kindly share this memo to me.