The ECCD Council releases Advisory No. 8 series of 2022 for everyone’s guidance on the conduct of the Safe Reopening of Early Childhood Education (ECE) and implementation of the Suggested Calendar of Activities for School Year 2022-2023.
Recognizing the urgent need to safely reopen ECE services to mitigate further development and learning loss, the ECCD Council, with technical inputs from the Department of Health (DOH) and the Department of the Interior and Local Government (DILG), through The Guidelines for the Safe Reopening of ECE During the COVID-19 Pandemic (Attachment 1). This set of guidelines will ensure that the safe reopening of ECE is well-planned, adequately resourced, and coordinated among different stakeholders at the national and local levels.
It is highly recommended that National Child Development Centers (NCDCs) and Child Development Centers (CDCs) start the SY 2022-2023 on September 5, 2022 and end on July 7, 2023. Specific center activities shall also be implemented as indicated in the Calendar of Activities for SY 2022-2023 (Attachment 2). Private Learning Centers (PLCs) may also adopt the recommended school calendar.
Early Learning Programs shall primarily be implemented through an in-person/face-to-face modality. Alternative Delivery Modes and class schedules shall be planned and implemented by the NCDC/CDC/PLC depending on the needs of the children and their families.
In order to prepare and be able to cope with the transition, it is recommended that the NCDC/CDC/PLC in coordination with the Barangay LGU/ School Administration conducts an orientation on the Safe ECE Reopening at least two weeks before the start of classes.
In preparation for the opening of classes, it is highly encouraged to conduct Bayanihang Bulilit to gather people in the community to engage in ECCD activities and services (e.g., Refurbishment of NCDC/CDC/PLC and Ensuring that Health and Safety facilities and supplies are in place).
For clarifications or inquiries, you may contact us through helpdesk@eccdcouncil.gov.ph or telephone numbers (02) 8571-4615/8571-6590.
For your guidance and implementation.
Table of Contents
ECCD Council Advisory No. 8 Series of 2022
Guidelines for the Safe Reopening of Early Childhood Education in the Philippines During the COVID-19 Pandemic
Background/Rationale
The first five (5) years are the most crucial years of brain development; thus, the importance of unhampered early childhood education (ECE) is given utmost priority by the State, in recognition of the Constitutional and statutory rights of the child, as provided in par. (3), Section 3, Article XV of the 1987 Constitution, and further embodied in Republic Act No. 10410, otherwise known as the Early Years Act (EYA) of 2013. ECE prepares the child for school, but more importantly, contributes to the physical, social, mental, and emotional well-being and development of children.
The COVID-19 pandemic has resulted in disruption of children’s education and the adverse effects of school/ECE closures on children’s safety, well-being, and learning have been recognized. The impact of closures extends beyond disruption to education and carries multiple, secondary risks to vulnerable children (e.g., children with delays and disabilities) and children from low-income households. Schools and ECE closures result in damage to children’s social, psychological, and educational development, as well as lost income and productivity in adults who cannot work because of childcare responsibilities.
Global data show that reopening of schools are not the main drivers of COVID-19 transmission and children of primary school age and younger appear to be less likely to be infected and less likely to pass on the infection to others (WHO and UNICEF, 2021). In the Philippines, children 0-4 years old comprise a very small proportion (1.1% female, 1.3% male) of total reported cases (DOH COVID-19 Tracker, 2022).
Recognizing the urgent need to safely reopen ECE services to mitigate further development and learning loss, the ECCD Council has adopted the Guidelines for the Safe Reopening of ECE. This set of guidelines will ensure that the safe reopening of ECE in low-risk areas is well-planned, adequately resourced, and coordinated among different stakeholders at national and local levels.
Objectives, Scope and Definition of Terms
Overall Goal and Objectives
The safe reopening of ECE shall have the following goal and specific objectives:
Goal: Children 0-4 years old shall have access to quality in-person/face-to-face ECE services in a safe and conducive learning environment.
Specific Objectives:
- Improve the capacity of LGUs, with focus on Municipality/City Local Government Units (M/CLGUs) in risk-informed planning, implementation, and monitoring of safe reopening of ECE;
- Uphold a safe learning environment in NCDCs/CDCs/PLCs and other ADM of ECE while children are enjoying and learning; and
- Strengthen the collaboration with clear responsibilities among different key stakeholders at the barangay, municipal/city, provincial and national levels.
Scope
This set of guidelines shall provide guidance on the standards and mechanisms for the safe reopening of ECE which aims to ensure that children are experiencing and enjoying development and learning activities together with some of their peers in a safe and conducive environment. This set of guidelines shall be implemented in National Child Development Centers (NCDCs), Child Development Centers (CDCs), and other alternative delivery modes (ADM) of ECE in low-risk municipalities and cities. This also applies to Private Learning Centers (PLCs)/preschools registered with the Securities and Exchange Commission (SEC) and has secured a Permit to Operate from the Office of the Mayor.
This set of guidelines also cover the roles and responsibilities of key stakeholders from different sectors across governance levels to ensure effective, efficient, and safe implementation of in-person/face-to-face ECE.
Definition of Terms
Barangay Health Emergency Response Teams (BHERTs), a community organization tasked in monitoring and controlling further community transmission of COVID-19 in the barangay.
Center-Based Program implemented in an Alternative Venue. An alternative delivery mode for the learning continuity plan for young children during emergency situations.
In this guideline, Child Development Teacher/Child Development Worker refers to ECCD service providers teaching in NCDCs, CDCs and PLCs.
Disaster Risk Reduction and Management Office at the national, regional, and local levels are the country’s disaster management coordination structure as mandated by RA 10121 or the Philippine Disaster Risk Reduction and Management Act.
Early Childhood Education (ECE) includes preschools, kindergartens, and other early childhood development centers, which are designed to include educational content for children aged 3 years up to the start of primary education, often around age 6. In this set of guidelines, ECE refers to the education of 3-4 years old.
The Inter-Agency Task Force on Emerging Infectious Diseases (IATF-EID or simply the IATF) is a task force organized by the executive of the Philippine government to respond to affairs concerning emerging infectious diseases in the Philippines.
The IATF-EID was created through Executive Order No. 168 as the government’s instrument to assess, monitor, contain, control, and prevent the spread of any potential epidemic in the Philippines.
Refers to the separation of ill or infected persons from others to prevent the spread of infection or contamination.
Refers to separating someone with confirmed COVID-19 or symptoms to prevent contact with others or reduce the risk of transmission. Medical isolation ends when someone meets pre-established clinical, time-based, and/or testing criteria for release from isolation in consultation with clinical health providers and public officials. This does not refer to punitive isolation for behavioral infractions within the custodial setting.
Refers to an area with a two-week growth rate of zero (TWGR) or below and an Average Daily Attack Rate (ADAR) of less than one (1). The TWGR refers to the growth in cases in the last two weeks, while the ADAR refers to the attack rate based on newly reported cases in the past two weeks (consistent with the latest Interagency Task Force quarantine/alert level classification).
Protective Personal Equipment (PPE)- refers to protective garments or equipment such as but not limited to face masks, face shields, and gloves, that must be worn by individuals to increase personal safety from infectious agents or to minimize exposure to hazards that may cause infection.
Refers to the separation and movement restrictions of people who were exposed to a contagious disease to see if they become sick.
Operational Framework and Guiding Principles for Safe Reopening of ECE
Operational Framework
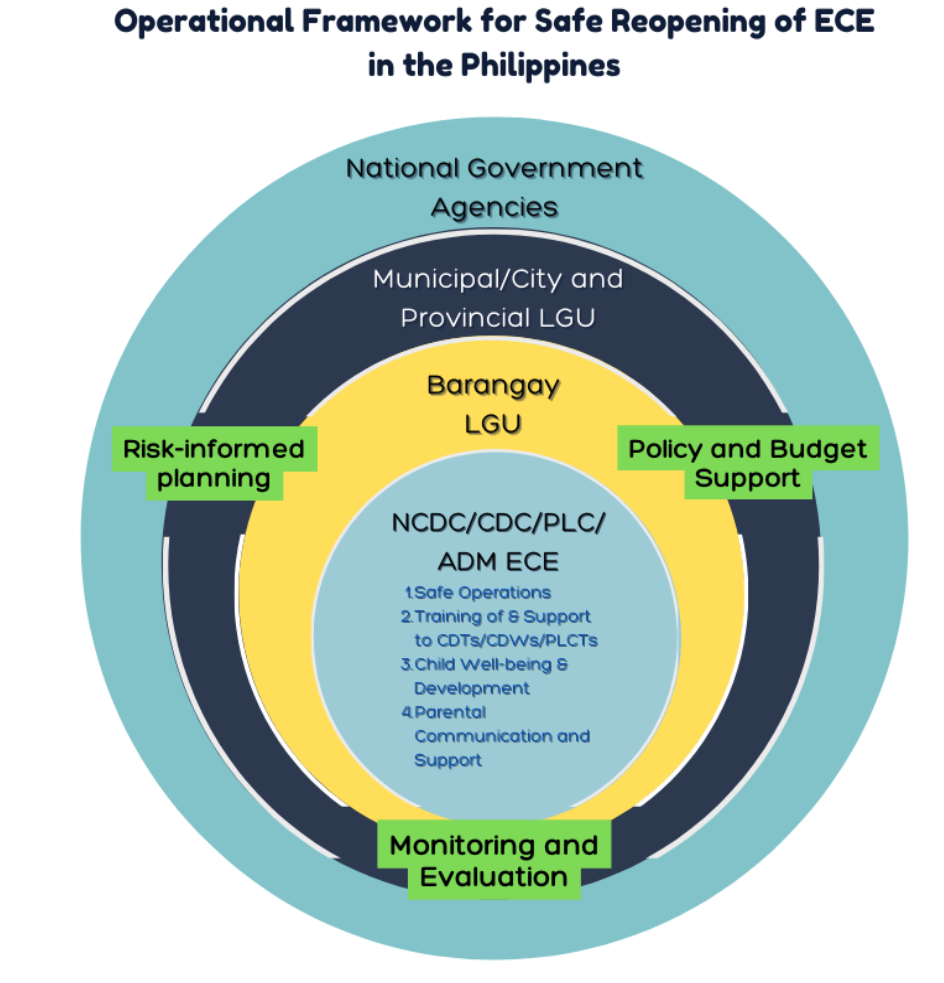
The Operational Framework for the Safe Reopening of ECE in the Philippines is anchored on the Framework for Reopening Schools as well as Global Guidance on Reopening in ECE Setting by the World Bank, UNESCO, and UNICEF.
The Framework shall focus on the following four (4) dimensions at the NCDC/CDC/PLC/ADM of ECE level: a) Safe Operations; b) Training of and Support to Child Development Teachers (CDTs)/Child Development Workers (CDWs)/Private Learning Center Teachers (PLCTs); c) Child Well-Being and Development; and d) Parental Communication and Support. Risk-informed planning, with policy and budget support, and strong monitoring and evaluation mechanisms at various governance levels are imperative to create an enabling environment to support each and across all dimensions. Figure 1 shows the Operational Framework for Safe Reopening of ECE in the Philippines.
Figure 1. Operational Framework for Safe Reopening of ECE in the Philippines
Key Guiding Principles
Towards addressing development and learning losses among young children in a safe environment, the safe reopening of ECE shall be guided by the following key principles:
Principle 1: Risk-informed planning at the LGU level is non-negotiable. Planning for the safe reopening of NCDCs/CDCs/PLCs/ADM of ECE shall be risk-informed and shall be specific to the LGU context using public health and social and economic data. The best interest of the child and overall public health considerations shall guide the timing of ECE reopening and the decision for re-closure.
Principle 2: Relevant policies and budget allocation shall be put in place. Effective safe reopening of NCDCs/CDCs/PLCs/ADM of ECE shall be ensured when relevant policies with adequate funding are in place prior to reopening, during reopening, and re-closure. The budget shall be allocated for infection prevention control measures and for improving the quality of ECE services.
Principle 3: Involvement of different stakeholders is imperative. The involvement of key stakeholders from health and nutrition, early education, social welfare, and disaster-risk reduction is crucial for a successful and safe ECE reopening. A coordinated and integrated approach shall be pursued to ensure children’s holistic needs are met when they return to ECE setting and in the event of re-closure. Key stakeholders at the national, provincial, municipal/city, and barangay levels, including mothers, fathers, and other caregivers of young children shall be involved in planning, implementing, and monitoring activities.
Principle 4: Training and support shall be provided to CDTs/CDWs/PLCTs. The CDTs/CDWs/PLCTs have a crucial role in providing a safe and inclusive environment for development and learning. They shall be trained prior to reopening and that their well-being, health, and safety are supported when NCDCs/CDCs/PLCs/ADM of ECE reopen.
Principle 5: Pedagogy shall be strengthened while ensuring that children are protected while engaging in play and learning. CDTs/CDWs/PLCTs shall be supported so that safe and developmentally-appropriate practices are effectively implemented for the continuous development and learning of young children. Measures shall be put in place to protect children while engaging in play and learning.
Principle 6: Prevent disease transmission and establish procedures if CDT/CDW/PLCT, children and their families become unwell. Regular monitoring of the health status of children and their families, CDTs/CDWs/PLCTs, and parent/center volunteers shall be pursued and procedures and measures to prevent disease transmission shall be put in place.
Principle 7. Plan ahead to support CDTs/CDWs, children and mothers, fathers, and other caregivers in the event of re-closure. To ensure continuity of development and learning of young children, the LGU through the Local Social Welfare and Development Office (LSWDO) shall build the capacity of the CDTs/CDWs and mothers, fathers, and other caregivers in the implementation of alternative modalities of delivering ECE services (e.g., Center-Based Program implemented in an Alternative Venue or CBPAV) in the event of re-closure. This shall be linked to the LGU Development Plan, Local Disaster Risk Reduction and Management Plan, and Comprehensive Emergency Plan for Children.
Key Stakeholders and their Roles
To ensure effective, efficient, and safe implementation of ECE reopening, the following major stakeholders at the national, sub-national, and LGU levels, with their respective roles are hereby delineated:
National level
1. Early Childhood Care and Development (ECCD) Council
The ECCD Council shall:
a. Be responsible for developing national policies and guidelines in the implementation of safe ECE reopening in close coordination with the Department of Health (DOH) and Department of the Interior and Local Government (DILG);
b. Have the oversight responsibility in monitoring LGU’s compliance to national policy and guidelines for the safe ECE reopening including data gathering of NCDCs’/CDCs’ profiles that have reopened;
c. Provide technical assistance to capacitate LGUs and ECCD service providers in the implementation of safe ECE reopening; and
d. Provide informational and advocacy materials on strategies or measures to ensure implementation of minimum public health standards.
2. Department of Health (DOH)
The DOH shall:
a. Be responsible for providing national guidance to ensure that health and safety protocols are always strictly observed by the NCDCs/CDCs/PLCs/ADM of ECE to ensure the safety of children;
b. Work closely with ECCD Council to provide timely updates on public health standards to be observed in educational settings; and
c. Provide informational and advocacy materials on strategies or measures to ensure implementation of minimum public health standards.
3. Department of the Interior and Local Government (DILG)
The DILG shall:
a. Work closely with ECCD Council to provide technical inputs and expertise on good governance, local government development, and other matters related to the safe reopening of NCDCs/CDCs/PLCs/ADM of ECE for children 3-4 years old;
b. Provide technical assistance, in partnership with the Regional Sub-Committee for the Welfare of Children (RSCWC), to improve/strengthen local governance in the context of the COVID-19 pandemic, from risk-informed planning to monitoring of LGUs’ programs to fulfill the rights of children to survival, development, participation, and protection;
c. Ensure that there is biological sex, age, disability status, and ethnicity disaggregated database of children and their access to education in line with the functions of the Barangay Council for the Protection of Children (BCPC); and
d. Ensure and advocate LGU compliance in increasing coverage of children 3-4 years old and ensuring the presence of ECCD services in all barangays through the Annual Child Friendly Local Governance Audit (CFLGA) and Council for the Welfare of Children (CWC).
4. Department of Social Welfare and Development (DSWD)
The DSWD shall:
a. Provide technical assistance to LGUs to ensure that the delivery of social services, particularly the Supplementary Feeding Program and Family Education Programs, are compliant with the minimum public health standards; and
b. Support CDTs/CDWs in acquiring competencies and continuous professional development through the different levels/tiers of providing capability-building initiatives aligned with the ECCD Council Training Framework.
Sub-national level
1. Provincial Disaster Risk Reduction and Management Office (PDRRMO) shall be responsible for implementing the local recovery plans, for the prevention, detection, isolation, treatment, and reintegration of people who are COVID-19 positive.
2. Provincial Social Welfare and Development Office/Provincial ECCD Office (if applicable) shall:
a. Provide close coordination and monitoring of the implementation of safe ECE reopening in M/CLGUs in the province including data gathering of NCDCs’/CDCs’ profiles that have reopened;
b. Provide technical assistance to M/CSWDO/ECCD Office (if applicable) in orienting CDTs/CDWs on the SOP;
c. Provide funding support to the M/CLGUs in implementing safe ECE reopening; and
d. Allocate funding and procurement of necessary items (e.g., Water, Sanitation, and Hygiene – WASH kits, sanitation facilities, etc.) to support the implementation of safe NCDC/CDC reopening aligned with COA and DBM procurement law/guidelines.
3. Provincial Health Office (PHO) shall monitor and provide technical assistance in ensuring the delivery of quality health and nutrition ECCD services at the M/C/BLGU levels.
LGU level
1. Municipal/City (Highly Urbanized City /Independent Component City /Component City)
1.1. Municipal/City Disaster Risk Reduction and Management Office (M/CDRRMO) shall develop risk-informed plans with strict adherence and alignment to the implementation of the SOP, along with other policies issued by the national and local IATF (Refer to Section VI.A. for specific guidance on the preparation of Risk-informed Plan). The development of the risk-informed plans shall include but not be limited to the following tasks:
a. Provision of funding support to the barangays and NCDCs/CDCs implementing the safe ECE reopening;
b. Be responsible for making and communicating its decisions to NCDCs/CDCs/PLCs for the appropriate actions/measures in ECE reopening and decisions on granular lockdowns and reopening of the area; and
c. Allocation of funds for, but not limited to the following activities and procurement of necessary items to support the implementation of safe ECE reopening aligned with COA and DBM procurement law/guidelines:
i. Provision/improvement of water, sanitation, and hygiene facilities; and a stockpile of cleaning and disinfecting supplies, soap, handwash, toothbrush, toothpaste, and temperature scanner;
ii. Provision of a sufficient supply of PPEs (e.g., face mask) to CDTs/CDWs and volunteers;
iii. Provision of support to CDTs/CDWs in facilitating developmentally appropriate and stimulating learning activities in a safe environment;
iv. Communication support and financial allowance for CDTs/CDWs to ensure that proper messages are disseminated in the community, including training of LGU stakeholders and CDTs/CDWs on proper messaging on COVID-19 and safe reopening of NCDCs/CDCs;
v. Training and support for parents/caregivers, especially fathers and other male caregivers, on topics including health protocols, parenting skills, and facilitating development and learning activities at home;
vi. COVID-19 Vaccination of CDTs/CDWs; and
vii. COVID-19 testing of CDTs/CDWs based on the existing DOH testing protocol prioritizing those who have flu-like symptoms and symptomatic close contacts.
d. Conduct periodic monitoring of compliance of NCDCs/CDCs/PLCs and BLGUs with the set of guidelines.
1.2. Municipal/City Local Council for the Protection of Children (LCPC) shall:
a. Provide close coordination, oversight, and monitoring of the implementation of the safe ECE reopening;
b. Facilitate the coordination and partnership with stakeholders (i.e., parents, teachers, child-led or youth group CSOs) and communities in the implementation of the set of guidelines;
c. Support the BLGUs in activating the BCPC and put in place proper coordination with the Barangay Health Emergency Response Team (BHERT) as part of contingency planning in worst-case scenarios; and
d. Conduct an orientation prior to the reopening of ECE to the members of the BCPC and other key community stakeholders on the existing health and safety protocols, mechanisms, and procedures needed in the safe reopening of ECE.
1.3. Municipal/City Social Welfare and Development Office (M/CSWDO) or ECCD Office /Division/Department (if applicable) shall:
a. Provide technical assistance to CDTs/CDWs on safe and quality ECE operations;
b. Facilitate barangay level coordination and program implementation;
c. Communicate policies/program updates on Safe ECE Reopening from ECCD Council and relevant National Government Agencies to the LCPC;
d. Provide technical assistance and training on the set of guidelines together with M/CHO, particularly on health and safety protocols. Moreover, the M/CSWDO/ECCD Office/Division/Department shall provide technical assistance/training to CDTs/CDWs in enriching development and learning activities at the center and in alternative venues in the event of re-closure;
e. Mobilize existing local/deputized ECCD focal persons in providing technical assistance through training the trainers and monitoring quality implementation of play-based activities adhering to minimum health and safety protocols to support CDTs/CDWs in designing activities in NCDCs/CDCs;
f. Provide quality assurance and technical assistance and monitoring to ensure that CDTs/CDWs are able to satisfactorily provide a safe learning environment to children;
g. Train and mentor CDTs/CDWs on providing psychosocial support to both children and their parents/caregivers using readily available resources/ materials (e.g., DRRM, MHPSS materials);
h. Train CDTs/CDWs on how to support parents/caregivers in conducting ADM of ECE such as CBPAV and the home-based programs should the NCDCs/CDCs need to be re-closed; and
i. Create a pool of trained CDTs/CDWs and volunteers who can cover for CDTs/CDWs when they are sick.
2. Barangay Level
2.1. Barangay Council for the Protection of Children (BCPC) shall:
a. Be responsible for the safe reopening of ECE, including, but not limited to linking with BHERTs and providing support (i.e., providing transportation to and from the NCDC/CDC, providing health and sanitation supplies) to vulnerable groups (i.e., children with disabilities, children belonging from IP communities);
b. Allocate funding and procurement of necessary items (e.g., Water, Sanitation, and Hygiene – WASH kits, sanitation facilities, etc.) to support the implementation of safe NCDC/CDC reopening in the barangay aligned with COA and DBM procurement law/guidelines;
c. Utilize the COVID-19 Referral System of the B/M/CLGU in coordination with the CDT/CDW and BHC/BHERT when a child shows flu-like symptoms during in-person sessions;
d. Conduct an orientation prior to the reopening of ECE to CDTs/CDWs, volunteers, mothers, fathers, other caregivers, and other key community stakeholders on the eligibility for participation, existing protocols, mechanisms, and set of guidelines on the safe reopening of ECE, and to allow parents/caregivers to help children to mentally and emotionally adapt and cope with the transition; and
e. Assist the LCPC in implementing ECCD initiatives.
2.2. Barangay Health Units (BHU)/ Centers (BHC) / Barangay Health Emergency Response Team (BHERT) shall:
a. Utilize the COVID-19 Referral System of the LGU in coordination with the CDT/CDW when a child shows flu-like symptoms during in-person sessions;
b. Assist in the implementation of vaccination campaigns and shall encourage parents whose children have missed vaccines to bring their children to the local health offices or private/NGO providers for the completion of vaccines. As part of regular health screening, the LGU shall also identify and refer children who are at-risk for dental problems and nutritional deficiencies;
c. Ensure that COVID-19 patients in quarantine are provided with food and necessities. Barangay Health Emergency Response Teams (BHERTs), which are composed of, but are not limited to, barangay health workers and designated barangay kagawads, play a crucial role in preventing the transmission of the virus by initiating contact tracing and monitoring household members or close contacts of confirmed COVID-19 patients for the possible onset of symptoms;
d. Continue working with the BHU/BHC and local health office during safe ECE reopening, and manage the patient navigation of COVID-19 suspects and their contacts among families which may include those with 3-4 years old children; and
e. Provide health promotion and education interventions, as well as primary health care, infection prevention and control messages in collaboration and partnership with the Sangguniang Kabataan (SK) Councils, to counter misinformation, stigma, and discrimination against COVID-19 patients.
2.3. CDTs/CDWs and PLCTs (whichever is applicable) shall:
a. Primarily be responsible for the children’s development and safety. They shall participate in BLGU planning for safe reopening and re-closure of NCDCs/CDCs and ensure strict implementation of health and safety protocols;
b. Utilize the COVID-19 Referral System of the LGU in coordination with the BHC/BHERT when a child shows flu-like symptoms during in-person/face-to-face sessions;
c. Maintain consistent and regular communication with mothers, fathers, and other caregivers to ensure that they also observe the protocols at home and in the community, and receive materials and messages on good health and nutrition;
d. Continue to perform their role in addressing the development and learning loss of children through facilitating developmentally appropriate and play-based activities based on the National Early Learning Curriculum (NELC) and the results of the ECCD Checklist Child’s Record 2, and in monitoring the development of children in a safe and conducive environment;
e. Support mothers, fathers, and other caregivers in facilitating activities at home to complement the classroom learning, and during ECE closure;
f. Develop cohort-based scheduling for all the participants to limit transmission across groups;
g. Collect from parents the children’s vaccination records through the intake form; and
h. Maintain stockpiling and inventory of hygiene and disinfecting supplies, including disinfectants and soap, adequate water supply, and hand sanitizers in the center with support from the LGU.
2.4. Mothers, Fathers and other caregivers shall:
a. Work closely with CDTs/CDWs/PLCTs in monitoring the child’s progress. They shall facilitate children’s development and learning activities at home especially when NCDCs/CDCs/PLCs are closed;
b. Ensure that they follow health and safety protocols to prevent transmission of the virus at the center, at home, and in the community;
c. Be responsible for self-health monitoring and reporting;
d. Attend the orientation on the Safe Reopening of ECE at least two weeks prior to the reopening to help prepare children mentally, emotionally, and cope with the transition; and
e. Provide to CDT/CDW the child’s vaccination records by filling up the intake form.
Eligibility for Participation in the Safe ECE Reopening
NCDCs/CDCs
- The NCDCs/CDCs shall be preferably situated in municipalities and cities in low-risk areas. For areas in higher risk level classifications, proper risk assessment shall be conducted by the LGU prior to reopening; and
- The BLGU and M/CLGU shall have committed to reopening the NCDC/CDC through a resolution, executive order, or any supporting policy document stating an expression of commitment. This is to ensure that policies and budget shall be put in place, there are robust plans for reopening and eventual re-closure, where necessary, and mechanisms for rigorous monitoring of compliance with the set of guidelines are established.
Private Learning Centers (PLCs)/ Preschools
- PLCs shall be registered and preferably situated in municipalities and cities in low-risk areas; and
- PLCs shall have an: a) implementation plan for safe reopening including class program, class schedule, and health and safety protocols (e.g., testing capacity for personnel and arrangements for all learners and personnel attending in-person/face-to-face ECE); and b) contingency plan in case of school re-closures and reopening in the event of detected cases among learners or ECE personnel.
Child Development Teachers/Child Development Workers (CDTs/CDWs)/ Teacher Aide/ Parent/Center Volunteers
- They shall undergo a physical examination at the M/CHO prior to participation in the in-person/face-to-face ECE learning.
- They shall be physically fit and safe from potentially contracting and/or transmitting COVID-19 and preferably as follows:
- 64 years old and below;
- has access to public/private transportation that comply with health and safety protocols from and to the area of residence and NCDC/CDC; and
- ideally, reside within the municipality/city where the NCDC/CDC is located.
- They are highly recommended to be fully vaccinated prior to participation in in-person/face-to-face classes.
- They should be fully oriented on the distinguishing signs and symptoms of COVID-19 and shall be made aware of the local health referral system established by the local City or Municipal Health Office.
Children
- All children, including those with developmental delays and disabilities, belonging to Indigenous Peoples communities, and from disadvantaged areas should be given equal access and appropriate accommodation to voluntary in-person/face-to-face ECE;
- Participation of children in in-person/face-to-face ECE shall be voluntary in nature. ADM of ECE must be available for children based on the needs assessment conducted by the NCDC/CDC/PLC;
- It is recommended that they undergo regular primary care consults and have up-to-date routine immunizations; and
- It is preferable that children reside within the municipality/city where the NCDC/CDC/PLC is located and can walk or have access to regulated public or private transportation.
Guidelines on Safe ECE Reopening
Risk-informed Planning for Safe ECE Reopening
A risk-informed plan for safe reopening and assessment of the feasibility of implementing protective measures before reopening of NCDC/CDC/ADM of ECE based on the recommendations of national and subnational authorities shall be developed by the LGU as initiated by the M/CDRRMO. This plan shall include a risk-based assessment, communication strategies, and a contingency plans.
1. Risk-based Assessment
a. Assessing access of children to quality ECE through NCDCs/CDCs or alternative delivery modes;
b. Assessing availability and appropriateness of existing handwashing facilities and other sanitation supplies;
c. Assessing the capacity of CDTs/CDWs to implement play-based learning in a safe learning environment;
d. Assessing the needs of children living with or without health conditions and special needs, as well as health conditions of CDTs/CDWs; and
e. Assessing capacity to reduce the risk of transmission by limiting the number of children and CDTs/CDWs in contact with each other.
2. Communication Strategies
a. Ensuring the availability of telecommunications or local hotline/help desk for proper referral and coordination to facilities, hospitals, or LGUs;
b. Developing or adopting readily available clear and easy-to-understand key messages on COVID-19 and NCDC/CDC reopening to inform CDTs/CDWs, LGU stakeholders, and community members on how to cascade the message to mothers, fathers, and other caregivers and children;
c. Creating easily understandable and inclusive communication materials (i.e., PA system, illustrations-based, posters with braille) available in the centers and other establishments in the community that would remind children, mothers, fathers, and other caregivers on safety and health protocols. Available materials from DOH, ECCD Council, IATF-EID, WHO, and UNICEF among others posted online can be adopted/adapted for use by the BLGUs and NCDCs/CDCs/PLCs; and
d. Developing detailed protocols on hygiene measures, including handwashing with soap, respiratory etiquette, use of protective equipment, cleaning procedures for facilities, and safe food preparation practices in accordance with existing DOH policies
3. Contingency Plan
a. Decision points for NCDC/CDC suspension and resumption of in-person/face-to-face learning sessions;
b. Clear protocols for medical isolation and re-closure in the event of detected cases among CDTs/CDWs, volunteers, parents/caregivers, and children;
c. Arrangement with the parents/caregivers for the continuation of development and learning while the child is in isolation or until it is safe for the child to return to the center by implementing alternative modalities (e.g., CBPAV);
d. Continued communication with all learners and their parents/caregivers, especially those children with or at-risk for developmental delays and disabilities, and offer the appropriate coaching to parents/caregivers to support children’s development, learning, and well-being at home through monitoring/home visitations; and
e. Strategies for the reopening of centers after the suspension.
Center Operations
1. Traveling to and from the NCDC/CDC/PLC
a. CDT/CDW/PLCT, center volunteers, parents/caregivers, and children shall wear their masks on properly at all times, promoting safety and hygienic practices whenever they walk to the center or are taking public or private transportation.
2. Traffic management, Entrance, and Exit of CDTs/CDWs/PLCTs and Children
a. The NCDCs/CDCs/PLCs shall provide reminders for health and safety protocols through creative posters, signage, and community updates that are easy to understand, and preferably in other accessible formats (e.g., PA system, illustrations-based, posters with braille);
b. A designated drop-off/ pick-up area for children and a waiting area for parents/caregivers shall be in place;
c. The NCDCs/CDCs/PLCs shall strategically designate the use of a door for entry and exit. Entry and exit signages and floor markings to guide traffic flow may be used; and
d. The NCDCs/CDCs/PLCs may use visual cues to encourage physical distancing inside and outside the center whenever possible:
i. The CDT/CDW/PLCT may use markers to serve as visual cues for children and parents in designated areas;
ii. The CDT/CDW/PLCT ensures that the center shall be free of clutter; and
iii. The NCDC/CDC/PLC shall use an appropriate number of chairs and tables depending on the number of children per session and other fixtures and furniture to provide adequate space for movement.
3. Arrival of CDTs/CDWs/PLCT, Parents/Caregivers, and Children
a. CDT/CDW/PLCT, parents/caregivers, and children shall wash their hands outside the center upon arrival;
b. CDTs/CDWs/PLCTs shall allow children who walk to the center to rest for 10-15 minutes upon arrival at the NCDC/CDC/PLC before temperature scanning;
c. CDTs/CDWs/PLCTs shall take children’s and parents’/caregivers’ temperatures using a forehead or wrist scanner. If the child’s body temperature is below 37.5C, the child shall be allowed to enter the center. If the child’s temperature is above 37.5C, the child shall be sent home or shall be referred to the BHU/BHC; and
d. Parents/caregivers shall fill out the attendance and visitors logbook to ensure the child’s security in the center.
4. Protective measures, hygiene and sanitation practices, and respiratory etiquette
a. The NCDC/CDC/PLC shall have the following provisions for infection prevention and control:
i. Sources of good airflow for adequate ventilation within the center
ii. Water for drinking, handwashing, general cleaning, and flushing the toilet;
iii. Toilet – at least one functional toilet with a lavatory with soap and water inside or nearby;
iv. Functional handwashing facility in strategic locations (e.g., near the entrance of the center, inside or outside the toilets);
v. Soap, oral health care, and other sanitation materials (e.g., hand sanitizer, alcohol, toothbrush/toothpaste);
vi. Schedule of supervised toothbrushing and handwashing activities;
vii. Placement of trash bins in strategic locations;
viii. Visuals signages on proper waste management practices near trash bins; and
ix. Visual cues that remind children to observe safety and hygiene practices.
b. For NCDCs/CDCs/PLCs that shall provide food, canteen staff/food handlers should be oriented on the Pinggang Pinoy and shall only serve healthful food;
c. Children, CDT/CDW/PLC Teachers, and volunteers shall be prohibited from eating together while facing one another. If there is a lack of space in the center to allow distancing during meals, eating shall be done in a manner where all individuals face in one direction and do not talk while their masks are off;
d. Ensure smoke-free environments in schools complementary to no-smoking policies and prevention education;
e. Prevent violence and injuries through healthy physical environments and anti-bullying policies;
f. Emergency Health Kits (e.g., gauze, cotton, plaster, antiseptic) shall be available in the center;
g. Stored PPEs (e.g., masks for children and adults, gloves) shall be available and accessible for all, including health care workers who will respond and assist if there are symptomatic children, volunteers, and parents/caregivers;
h. Children (2 years of age or older) and their accompanying adults shall wear masks when outside their homes and when around people who live outside of their household. Ensure that masks shall be worn correctly, consistently, and safely. Masks of proper size should be used to fully cover the nose and mouth of the child. Three-layer cloth masks or surgical masks may be used; masks with valves or other configurations are not recommended;
i. A mask shall not be recommended in the following situations: if the child has difficulty breathing when wearing it; if the child has a cognitive or respiratory impairment giving them a difficult time tolerating the mask; if the mask is a possible choking or strangulation hazard; and if wearing a mask causes the child to touch their face more frequently;
j. CDT/CDW/PLCT, volunteers, and parents/caregivers shall properly dispose of used facemasks by placing them in resealable plastic bags and throwing them in an enclosed garbage container; and
k. Visitors with approved or cleared appointments shall follow health protocols and screening, present/provide their identification card, and fill out the visitor’s logbook.
5. Daily monitoring of health status of CDT/CDW/PLCT, volunteers, parents/caregivers, and children, referral of and provision of support to suspected/confirmed COVID-19 cases
a. The NCDC/CDC/PLC shall enforce the “Stay at Home if Unwell” Policy among CDT/CDW/PLCT, volunteers, parents/caregivers, and children;
b. Parents shall notify the CDT/CDW/PLCT if family members show flu-like symptoms. In such cases, the child shall stay home until the improvement or resolution of symptoms;
c. The CDT/CDW/PLCT shall keep an updated attendance sheet of the class with remarks on the incurred absence/s of each child;
d. The center shall implement the referral mechanism for COVID-19 when individuals who manifest symptoms while in the NCDC/CDC/PLC shall immediately be brought to the BHU/BHC for medical assessment and referral to appropriate authorities and/or facilities;
e. The confidentiality of information on confirmed COVID-19 cases in the NCDC/CDC/PLC shall be ensured by the CDT/CDW/PLCT; and
f. Quarantine and isolation protocols shall be aligned with the latest national guidelines. Repeat testing and/or medical certification shall not be required for the safe return to the NCDC/CDC/PLC. Time-based isolation is sufficient, provided the affected individual remains asymptomatic.
6. Scheduling of Sessions, Development, and Learning of Children
a. The scheduling of learning sessions shall be based on the assessment of center needs (e.g., the risk level of the LGU, the total number of children enrolled, number of sessions offered, number of children per session);
b. The NCDC/CDC/PLC shall adopt the cohort approach where a number of children stay in the same group/class/session with the same CDT/CDW/PLCT, without mixing with other groups/classes/sessions;
c. The CDT/CDW/PLCT shall administer the ECCD Checklist to the children on a one-to-one basis to determine the status of development of children at least twice within the year (a month after the reopening of the NCDC/CDC/PLC, and six months after the first assessment);
d. The CDT/CDW/PLCT shall adapt to the National Early Learning Curriculum wherein healthy habits and safety protocols are incorporated into the routine activities;
e. The maximum number of children per session shall be based on the classroom size that would allow children to move and engage in developmentally appropriate and play-based activities;
f. Children shall be assigned to their permanent chairs/tables during sessions;
g. Children shall be taught to responsibly dispose of their used items (e.g., face masks);
h. The CDT/CDW/PLCT shall discuss and introduce non-contact greetings that are fun and child-friendly with children and staff;
i. The CDT/CDW/PLCT shall utilize play-based activities and multi-sensorial learning experiences;
j. The CDT/CDW/PLCT shall use creative educational/instructional practices to ensure inclusive, play-based, and developmentally-appropriate learning experiences around the pandemic situation;
k. The CDT/CDW/PLCT shall be encouraged to implement learning activities outdoors as much as possible. Consider adapting the curriculum, lesson plans, and instruction for outdoor delivery (e.g., use outdoor equipment and nature as teaching/learning materials);
l. The CDT/CDW/PLCT shall conduct activities that promote gender equality and inclusion of children with disabilities, migrant, displaced, and returnee children, focusing on values and attitudes that contribute to peacebuilding and social cohesion to respond to increased stigma and discrimination in the context of COVID-19;
m. The CDT/CDW/PLCT shall introduce the concept of self-help while encouraging children to maintain individual personal hygiene such as washing hands, using hand sanitizer, brushing their teeth after meals, using a tissue when coughing or sneezing, throwing their trash, avoiding putting toys/materials in their mouth, or touching their mouth/eyes after playing with toys, etc.; and
n. The CDT/CDW/PLCT, with support from parents/caregivers, shall continue to implement the Supplementary Feeding Program/Snack Time while observing health and safety protocols during this routine (e.g., children stay seated while eating).
7. Children’s Well-being and Development
a. The CDT/CDW/PLCT shall allow the parent/caregiver of children with disabilities (learning disability or physical disability) to stay in the classroom to assist their child;
b. The CDT/CDW/PLCT shall address and consider children’s emotions and concerns as this is important for their well-being;
c. The CDT/CDW/PLCT shall ensure young children receive support to channel emotions (verbalize, adapt their behaviors, and understand changes) while achieving significant learning and promoting mental health during the pandemic; and
d. The CDT/CDW/PLCT shall follow the protocol for Case Management of Child Victim of Abuse, Neglect, and Exploitation, whereby any cases shall be reported verbally or in writing to government agencies (e.g., LSWDO, BCPC, PNP, NBI, etc).
8. Disinfection and Waste Management
a. The CDT/CDW/PLCT, with the support of volunteers, shall disinfect before and after each session all frequently touched surfaces, such as door handles, tables, chairs, toys, supplies, light switches, door frames, play equipment, and teaching and learning aids used by children as well as common spaces such as learning areas, toilets, and kitchen;
b. The CDT/CDW/PLCT shall ensure that reading materials and wooden and plastic toys can be easily cleaned before the start or end of a session. They shall avoid mixing toys between groups of children before they are washed and/or disinfected. Soft toys made of fabric and stuffed with cotton and other materials which cannot be easily cleaned shall be stored for use when the pandemic ends;
c. The NCDC/CDC/PLC shall use disinfectants that are approved by the Philippine Food and Drug Administration (FDA) such as sodium hypochlorite recommended ratio of 0.1% (1000 ppm) by dissolving tsp of chlorine or 2 g to 2L of clean water for regular disinfection, and recommended ratio of 0.5% (5000 ppm) for body fluids by dissolving 1 tbsp of chlorine or 10 g to 2L of clean water; ethanol in all surfaces at a recommended ratio of 70-90%, or Hydrogen peroxide in all surfaces at a recommended ratio of >0.5%;
d. The CDT/CDW/PLCT, teacher aide, and parent/center volunteers shall dispose of used PPE in a separate leak-proof yellow trash bag container with a cover properly labeled as “Used PPE”. In case a yellow trash bag/container is not available, the NCDC/CDC/PLC shall dispose of all used PPE in a separate bag/container marked for infectious medical waste identifiable by the waste collector (e.g., yellow ribbon, yellow colored tag);
e. The NCDC/CDC/PLC shall treat the collected wastes with a chlorine solution (1:10) through disinfection or spraying; and
f. Disinfectants used in the NCDC/CDC/PLC shall be compliant with the DOH-FDA-approved preparation of disinfectants.
9. Heating, Ventilation, and Air-conditioning (HVAC)
a. Proper and adequate ventilation shall be maintained through different strategies depending on the risks and situations in a particular space. Adequate ventilation may be achieved through natural ventilation such as opening the windows and doors; and
b. Enclosed spaces with limited ventilation may entail higher monitoring equipment. Other options to increase ventilation include using exhaust fans and placing fans near windows. If feasible, adequate airflow can be measured through the use of monitoring devices with a target reading of 6 to 12 Air Change per Hour (ACH) and CO2 concentration below 1000ppm and taking into consideration the room size and capacity.
Monitoring and Evaluation
The implementation of this set of guidelines shall be monitored and evaluated at national and local levels to track the progress of the reopening of NCDCs/CDCs/PLCs/ADM of ECE and identify areas that can be improved and emerging good practices that can be replicated in similar settings.
Effectivity
This memorandum shall take effect immediately upon publication on the official website of the ECCD Council or in any national newspaper of general circulation.